
Muscle relaxants are a diverse group of medications used to relieve muscle spasms, spasticity, and associated musculoskeletal pain.
A muscle relaxant is a drug that affects skeletal muscle function and decreases the muscle tone. It may be used to alleviate symptoms such as muscle spasms, pain, and hyperreflexia. The term “muscle relaxant” is used to refer to two major therapeutic groups: neuromuscular blockers and spasmolytics. Neuromuscular blockers act by interfering with transmission at the neuromuscular end plate and have no central nervous system (CNS) activity. They are often used during surgical procedures and in intensive care and emergency medicine to cause temporary paralysis. Spasmolytics, also known as “centrally acting” muscle relaxant, are used to alleviate musculoskeletal pain and spasms and to reduce spasticity in a variety of neurological conditions. While both neuromuscular blockers and spasmolytics are often grouped together as muscle relaxant, the term is commonly used to refer to spasmolytics only.

What are the top 5 muscle relaxers?
The options will depend on your needs and other factors, but five commonly prescribed drugs are:
- baclofen (Lioresal)
- dantrolene (Dantrium)
- carisoprodol (Soma)
- clorzoxazone (Lorzon)
- methocarbamol (Robaxin)
List of Twenty Muscle Relaxant
Here is a list of 20 muscle relaxants, including both centrally acting and peripherally acting agents, as well as commonly used medications across various indications (spasticity, spasms, anesthesia, etc.):
Centrally Acting Muscle Relaxants
(Used for spasticity or musculoskeletal conditions)
- Baclofen – GABAB receptor agonist; spasticity
- Tizanidine – α2 -adrenergic agonist; spasticity
- Cyclobenzaprine – Tricyclic-like; acute muscle spasm
- Methocarbamol – CNS depressant; musculoskeletal pain
- Carisoprodol – CNS depressant; metabolized to meprobamate
- Metaxalone – CNS depressant; acute spasm
- Chlorzoxazone – CNS depressant; older agent
- Orphenadrine – Anticholinergic with analgesic properties
- Diazepam – Benzodiazepine; both spasm and spasticity
- Clonazepam – Benzodiazepine; occasionally used for spasticity
- Gabapentin – Anticonvulsant; off-label for spasticity
- Pregabalin – Similar to gabapentin; nerve pain + spasticity
- Valium (diazepam) – Common brand of diazepam
- Oxazepam – Short-acting benzodiazepine; rarely used for spasms
- Phenibut (in some countries) – GABAB agonist; not FDA approved
Peripherally Acting Muscle Relaxants
(Act at the neuromuscular junction or muscle fiber level)
- Dantrolene – Inhibits calcium release in skeletal muscle
- Botulinum toxin (Botox) – Blocks acetylcholine release
- Succinylcholine – Depolarizing neuromuscular blocker; anesthesia use
- Rocuronium – Non-depolarizing NMJ blocker; anesthesia use
- Vecuronium – Similar to rocuronium; used in surgery
Note: Some of these (like succinylcholine, vecuronium) are used only in surgical or ICU settings under anesthesia. Others (like carisoprodol) carry a high risk of abuse and dependence and are not first-line.
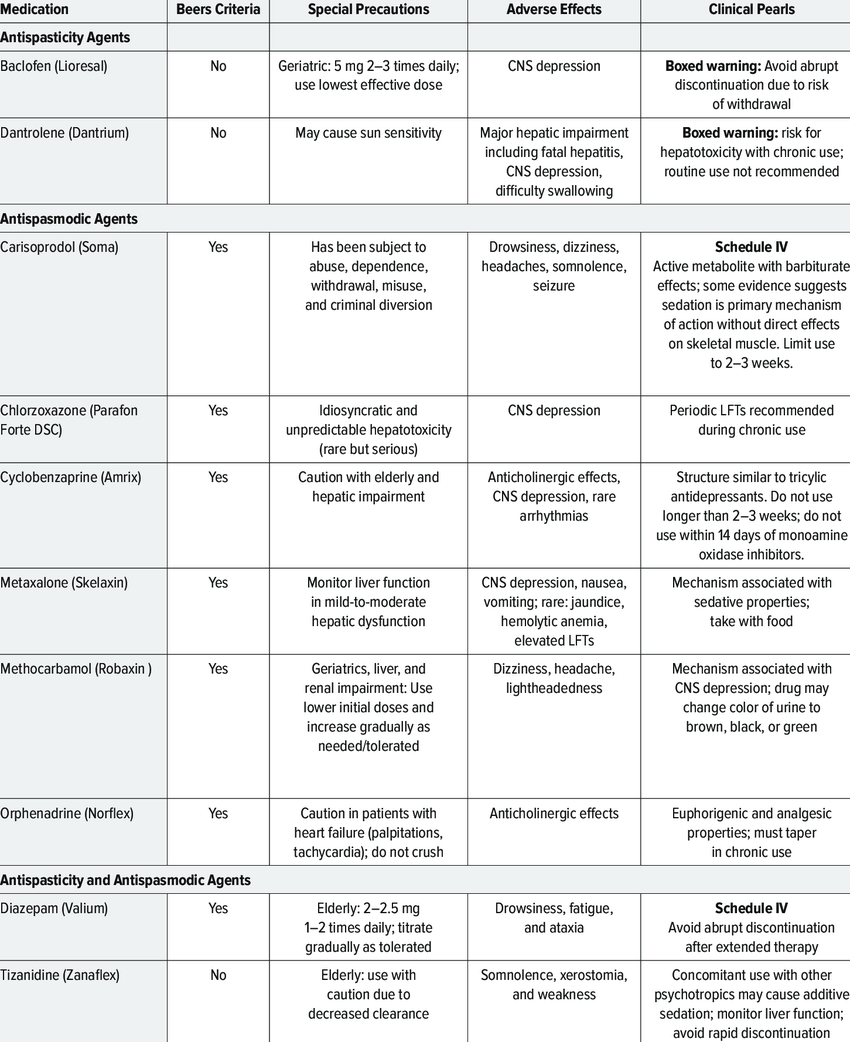
Types of Muscle Relaxants
Muscle relaxants are a diverse group of medications used to relieve muscle spasms, spasticity, and associated musculoskeletal pain. They can be broadly classified into two main categories based on their site of action and clinical usage:
A. Centrally Acting Muscle Relaxants
These work by depressing the central nervous system (CNS), reducing muscle tone and involuntary muscle activity.
i. For Muscle Spasms (Acute Musculoskeletal Conditions)
Commonly prescribed for acute back pain, injuries, or tension headaches.
| Drug | Mechanism | Notes |
|---|---|---|
| Cyclobenzaprine | Related to tricyclic antidepressants; reduces tonic somatic motor activity | Sedating; most commonly prescribed |
| Methocarbamol | CNS depressant | Less sedating than cyclobenzaprine |
| Carisoprodol | Metabolized to meprobamate (a sedative) | Abuse potential; Schedule IV drug |
| Metaxalone | Exact MOA unclear; CNS depressant | Milder side effects |
| Chlorzoxazone | CNS depressant | Older; less commonly used |
| Orphenadrine | Anticholinergic + antihistamine action | Also used for Parkinsonism tremor |
ii. For Spasticity (Neurologic Conditions)
Used for spasticity due to CNS injury (e.g., MS, spinal cord injury, cerebral palsy).
| Drug | Mechanism | Notes |
|---|---|---|
| Baclofen | GABAB agonist → inhibits spinal reflexes | Oral or intrathecal forms; watch for withdrawal |
| Tizanidine | α2-adrenergic agonist → inhibits motor neurons | Less sedating; hepatotoxic risk |
| Diazepam | Benzodiazepine → GABAA enhancer | Good for both spasm and spasticity; risk of sedation, dependence |
| Clonazepam | Similar to diazepam, longer acting | Useful in resistant cases |
| Gabapentin | Originally for seizures, also reduces spasticity | Off-label use |
| Dantrolene | Direct skeletal muscle relaxant (not CNS) | Only drug in class; used for malignant hyperthermia, spasticity |
B. Peripherally Acting Muscle Relaxants
Work directly at the neuromuscular junction or muscle fibers.
| Drug | Use | Mechanism |
|---|---|---|
| Botulinum toxin (Botox) | Focal spasticity, dystonia, cosmetic | Blocks ACh release at NMJ |
| Dantrolene | Chronic spasticity, malignant hyperthermia | Inhibits calcium release from sarcoplasmic reticulum |
Clinical Uses of Muscle Relaxants
- Acute low back pain
- Neck pain
- Fibromyalgia
- Spasticity from CNS lesions (MS, CP, stroke)
- Tetanus
- Temporomandibular joint disorders
- Adjunct in anesthesia (e.g., succinylcholine in intubation)
Mechanism of Muscle Relaxant
Because of the enhancement of inhibition in the CNS, most spasmolytic agents have the side effects of sedation and drowsiness and may cause dependence with long-term use. Several of these agents also have abuse potential, and their prescription is strictly controlled.
The benzodiazepines, such as diazepam, interact with the GABAA receptor in the central nervous system. While it can be used in patients with muscle spasm of almost any origin, it produces sedation in most individuals at the doses required to reduce muscle tone.
Baclofen is considered to be at least as effective as diazepam in reducing spasticity, and causes much less sedation. It acts as a GABA agonist at GABAB receptors in the brain and spinal cord, resulting in hyperpolarization of neurons expressing this receptor, most likely due to increased potassium ion conductance. Baclofen also inhibits neural function presynaptically, by reducing calcium ion influx, and thereby reducing the release of excitatory neurotransmitters in both the brain and spinal cord. It may also reduce pain in patients by inhibiting the release of substance P in the spinal cord, as well.
Clonidine and other imidazoline compounds have also been shown to reduce muscle spasms by their central nervous system activity. Tizanidine is perhaps the most thoroughly studied clonidine analog, and is an agonist at α2-adrenergic receptors, but reduces spasticity at doses that result in significantly less hypotension than clonidine. Neurophysiologic studies show that it depresses excitatory feedback from muscles that would normally increase muscle tone, therefore minimizing spasticity. Furthermore, several clinical trials indicate that tizanidine has a similar efficacy to other spasmolytic agents, such as diazepam and baclofen, with a different spectrum of adverse effects.
The hydantoin derivative dantrolene is a spasmolytic agent with a unique mechanism of action outside of the CNS. It reduces skeletal muscle strength by inhibiting the excitation-contraction coupling in the muscle fiber. In normal muscle contraction, calcium is released from the sarcoplasmic reticulum through the ryanodine receptor channel, which causes the tension-generating interaction of actin and myosin. Dantrolene interferes with the release of calcium by binding to the ryanodine receptor and blocking the endogenous ligand ryanodine by competitive inhibition. Muscle that contracts more rapidly is more sensitive to dantrolene than muscle that contracts slowly, although cardiac muscle and smooth muscle are depressed only slightly, most likely because the release of calcium by their sarcoplasmic reticulum involves a slightly different process. Major adverse effects of dantrolene include general muscle weakness, sedation, and occasionally hepatitis.
Other common spasmolytic agents include: methocarbamol, carisoprodol, chlorzoxazone, cyclobenzaprine, gabapentin, metaxalone, and orphenadrine.
Thiocolchicoside is a muscle relaxant with anti-inflammatory and analgesic effects and an unknown mechanism of action. It acts as a competitive antagonist at GABAA and glycine receptors with similar potencies, as well as at nicotinic acetylcholine receptors, albeit to a much lesser extent. It has powerful proconvulsant activity and should not be used in seizure-prone individuals.

Side Effects of Muscle Relaxant
Patients most commonly report sedation as the main adverse effect of muscle relaxants. Usually, people become less alert when they are under the effects of these drugs. People are normally advised not to drive vehicles or operate heavy machinery while under muscle relaxants’ effects.
Cyclobenzaprine produces confusion and lethargy, as well as anticholinergic side effects. When taken in excess or in combination with other substances, it may also be toxic. While the body adjusts to this medication, it is possible for patients to experience dry mouth, fatigue, lightheadedness, constipation or blurred vision. Some serious but unlikely side effects may be experienced, including mental or mood changes, possible confusion and hallucinations, and difficulty urinating. In a very few cases, very serious but rare side effects may be experienced: irregular heartbeat, yellowing of eyes or skin, fainting, abdominal pain including stomach ache, nausea or vomiting, lack of appetite, seizures, dark urine or loss of coordination.
Patients taking carisoprodol for a prolonged time have reported dependence, withdrawal and abuse, although most of these cases were reported by patients with addiction history. These effects were also reported by patients who took it in combination with other drugs with abuse potential, and in fewer cases, reports of carisoprodol-associated abuse appeared when used without other drugs with abuse potential.
Common side effects eventually caused by metaxalone include dizziness, headache, drowsiness, nausea, irritability, nervousness, upset stomach and vomiting. Severe side effects may be experienced when consuming metaxalone, such as severe allergic reactions (rash, hives, itching, difficulty breathing, tightness in the chest, swelling of the mouth, face, lips, or tongue), chills, fever, and sore throat, may require medical attention. Other severe side effects include unusual or severe tiredness or weakness, as well as yellowing of the skin or the eyes. When baclofen is administered intrathecally, it may cause CNS depression accompanied with cardiovascular collapse and respiratory failure. Tizanidine may lower blood pressure. This effect can be controlled by administering a low dose at the beginning and increasing it gradually.
Muscle Relaxant Prescription Medications
Prescription medications are divided into two groups: antispasmodics and antispastics.
Antispasmodics are used to treat muscle spasms, and antispastics are used to treat muscle spasticity. Some antispasmodics, such as tizanidine, can be used to treat muscle spasticity. However, antispastics should not be used to treat muscle spasms.
Antispasmodics: Centrally acting skeletal muscle relaxants (SMRs)
Centrally acting SMRs are used in addition to rest and physical therapy to help relieve muscle spasms. They’re thought to work by causing a sedative effect or by preventing your nerves from sending pain signals to your brain.
You should only use these muscle relaxants for up to 2 or 3 weeksTrusted Source. The safety of longer-term use is not yet known.
While antispasmodics can be used to treat muscle spasms, they have not been shown to work better than nonsteroidal anti-inflammatory drugs (NSAIDs) or acetaminophen. In addition, they have more side effects than NSAIDs or acetaminophen.
The more common side effects of centrally acting SMRs include:
- drowsiness
- dizziness
- headache
- nervousness
- lowered blood pressure upon standing
You should talk to your doctor about the benefits and risks of these medications for the treatment of your muscle spasms.
List of centrally acting SMRs
| Generic name | Brand name | Form | Generic available |
|---|---|---|---|
| carisoprodol | Soma | tablet | yes |
| carisoprodol/aspirin | not available | tablet | yes |
| carisoprodol/aspirin/codeine | not available | tablet | yes |
| chlorzoxazone | Parafon Forte, Lorzone | tablet | yes |
| cyclobenzaprine | Fexmid, Flexeril, Amrix | tablet, extended-release capsule | tablet only |
| metaxalone | Skelaxin, Metaxall | tablet | yes |
| methocarbamol | Robaxin | tablet | yes |
| orphenadrine | Norflex | extended-release tablet | yes |
| tizanidine | Zanaflex | tablet, capsule | yes |
Antispastics
Antispastics are used to treat muscle spasticity. They should not be used to treat muscle spasms. These drugs include the following:
Baclofen
Baclofen (Lioresal) is a skeletal muscle relaxer used to relieve spasticity caused by MS. It’s not fully understood how it works, but it seems to block nerve signals from the spinal cord that cause muscles to spasm. Side effects can include drowsiness, dizziness, weakness, and fatigue.
Dantrolene
Dantrolene (Dantrium) is a skeletal muscle relaxer used to treat muscle spasms caused by spinal cord injury, stroke, cerebral palsy, or MS. It works by acting directly on the skeletal muscle to relax the muscle spasm. Side effects can include drowsiness, dizziness, lightheadedness, and fatigue.
Diazepam
Diazepam (Valium) is a benzodiazepine used to relieve muscle spasms caused by inflammation, trauma, or muscle spasticity.
It works by increasing the activity of a certain neurotransmitter to decrease the occurrence of muscle spasms. Diazepam is a sedative. Side effects can include drowsiness, fatigue, and muscle weakness.
List of Antispastics
| Generic name | Brand name | Form | Generic available |
|---|---|---|---|
| baclofen | Lioresal, Gablofen, Lioresal | tablet, injection | yes |
| dantrolene | Dantrium | tablet | yes |
| diazepam | Valium | oral suspension, tablet, injection | yes |
Muscle relaxants such as carisoprodol and diazepam can be habit-forming. Be sure to take your medication exactly as prescribed by your doctor.
Also, muscle relaxants depress your central nervous system (CNS), making it hard to pay attention or stay awake. While taking a muscle relaxant, avoid activities that require mental alertness or coordination, such as driving or using heavy machinery.
You should not take muscle relaxants with:
- alcohol
- CNS depressant drugs, such as opioids or psychotropics
- sleeping medications
- herbal supplements such as St. John’s wort
Talk to your doctor about how you can safely use muscle relaxants if you:
- are older than 65 years
- have a mental health problem or brain disorder
- have liver problems
Doctors can use certain medications to treat spasticity even when the drugs are not approved for that purpose by the U.S. Food and Drug Association (FDA). This is called off-label drug use.
The following drugs are not actually muscle relaxants, but they can still help relieve symptoms of spasticity.
Benzodiazepines
Benzodiazepines are sedatives that can help relax muscles. They work by increasing the effects of certain neurotransmitters, which are chemicals that relay messages between your brain cells.
Examples of benzodiazepines include:
- clonazepam (Klonopin)
- lorazepam (Ativan)
- alprazolam (Xanax)
Side effects of benzodiazepines can include drowsiness and problems with balance and memory. These drugs can also be habit-forming.
Gabapentin
Gabapentin (Neurontin) is an anticonvulsant drug typically used to relieve seizures. It may also help prevent pain responses associated with spasticity. Gabapentin is available in brand-name and generic versions.
OTC treatment is recommended as first-line therapy for muscle spasms caused by conditions such as acute lower back pain or tension headache. This means you should try OTC treatments before prescription medications.
OTC treatment options include nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, or a combination of both. Your doctor or pharmacist can help you choose an OTC treatment.
Nonsteroidal anti-inflammatory drugs (NSAIDs)
NSAIDs work byTrusted Source blocking your body from making certain substances that cause inflammation and pain. NSAIDs are available in generic and brand-name versions. They’re typically sold over the counter. Stronger versions are available by prescription.
NSAIDs come as oral tablets, capsules, or suspensions. They also come as chewable tablets for children. Side effects of these drugs can include upset stomach and dizziness.
Examples of NSAIDs include:
Acetaminophen
Acetaminophen (Tylenol) is thought to work by blockingTrusted Source your body from making certain substances that cause pain. Acetaminophen is available in generic and brand-name versions. It comes as immediate-release and extended release oral tablets and capsules, orally disintegrating tablets, chewable tablets, and oral solutions.
The more common side effects of acetaminophen can include nausea and upset stomach.
Studies show that certain compounds in cannabis could act as a muscle relaxant, including tetrahydrocannabinol (THC), the substance responsible for the psychoactive effects of marijuana.
However, research on the medicinal properties of cannabis are limited, as its cultivation, supply, and possession is still prohibited in many areas.
Therefore, more research is needed to understand whether cannabis or the compounds it contains could help ease muscle spasms or muscle spasticity.
You can often manage your muscle spasm or spasticity symptoms on your own, but in some cases, you may need medical advice or care. Be sure to call your doctor if you:
- have spasticity for the first time and don’t know the cause
- notice the spasticity is getting more severe, happening more often, or making tasks difficult
- have severe and frequent muscle spasms
- notice deformity of the parts of your body affected by muscle spasms
- have side effects from your muscle relaxant
- have a “frozen joint” due to contracture that decreases your range of motion or causes pressure sores
- have increasing discomfort or pain